Use of IC-Green® (indocyanine green for injection) in Minimally Invasive Surgery
Minimally Invasive Surgery (MIS), using small incisions to minimize trauma to normal tissues and adjacent organs, is now the preferred method of undertaking many surgeries.
The global minimally invasive surgical systems market is expected to grow at a Compound Annual Growth Rate of 10.9% from 2020 to 2025, driven by the rapidly increasing demand from the patients undergoing minimally invasive surgical procedures, increasing surgical need, and the surge in the prevalence of colorectal and other gastrointestinal diseases.1
New technological advancements, such as miniaturization of surgical equipment and development of surgical robots, have substantially increased the number of minimally invasive surgeries performed across the world.
Laparoscopic Cholecystectomy (Lap Chole)
Key Features
Laparoscopic Cholecystectomy is the gold standard for gall bladder surgery and is one of the most common surgeries undertaken worldwide. In the USA an estimated one million Lap Chole’s are undertaken each year, with an estimated 500,000 in Europe.2
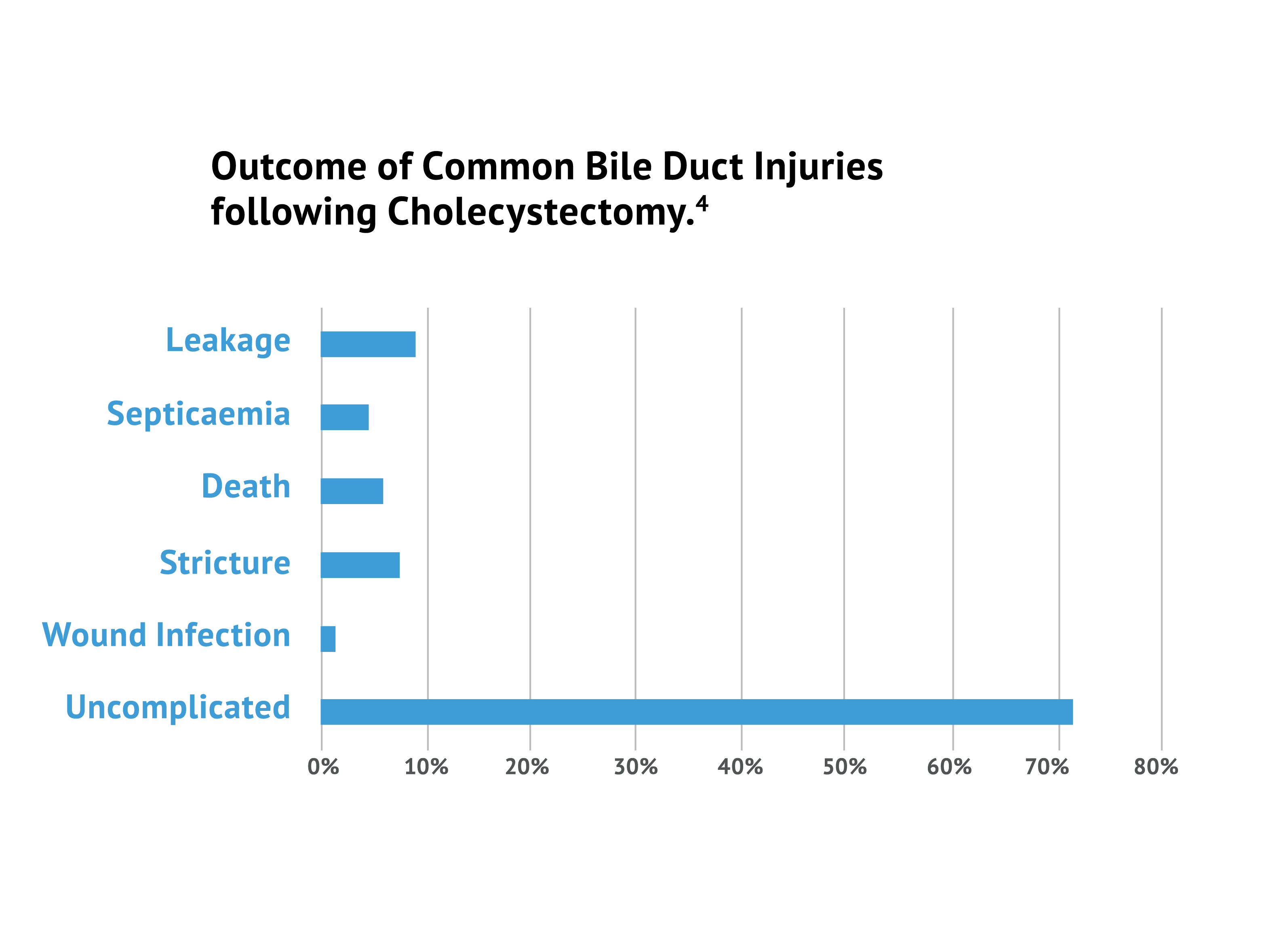
Whilst the incidence of Bile Duct Injury (BDI) is low at 0.5%, due to the considerable amount of surgeries, this becomes quite a significant number with thousands of resultant patients per year thus sustaining BDI’s, with severe and long term implications for their health.2 The primary cause of error in 97% of Lap Chole cases was a visual perception illusion, which is one of the major drawbacks of an MIS approach.3

ICG fluorescence imaging during Laparoscopic Cholecystectomy (Lap Chole) surgery reduces BDI injuries and improves patient outcomes
The primary cause of error in 97% of cases was a visual perception illusion.3
Surgeons had a 3-fold improvement in ability to visualize critical bile duct structures using ICG.4
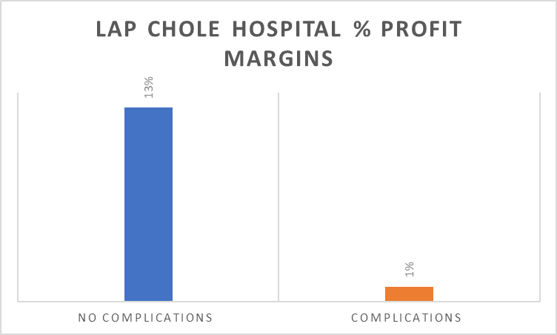
Profit margins at hospitals drop from 13% to 1% when complications in lap chole surgeries occur.5

ICG Guided Cholecystectomy vs X-Ray Cholangiography
X-Ray Cholangiography has been used in the past to overcome this visualization problem. However it has drawbacks that are not apparent with Indocyanine Green (ICG) use.
Colorectal Surgery
Colorectal surgery frequently involves bowel resection with restoration of the alimentary tract by anastomosis. Indocyanine green (ICG) fluorescence imaging has proven to be an effective tool to assess anastomotic perfusion. Its use for the prevention of anastomotic leaks (AL) has been gaining popularity, with accumulating data on lower leak rates with (ICG) fluorescence guided surgery.9
Most common methods used to evaluate the perfusion status of the colon has been to visually observe the change in color of the colon wall with the surgeon’s naked eye and to carefully observe the pulse of the colon wall.
However, these methods are subjective and not always accurate.
Reported rates of anastomotic leakage vary from 3-6% in experienced colorectal surgeons and 3-25% overall.10 Combining the use of ICG with a near-infra red (NIR) laparoscopic camera system offers the surgeon the possibility of an objective, real-time assessment of blood flow to the colon.
| Procedure | Leak Rate | Mortality |
|---|---|---|
| Colon Resection | 2.7% | Up to 15% |
| Rectal Resection | 5-20% | Up to 10% |
| Esophagectomy | 4-25% | Up to 50% |
| Total/Partial Gastrectomy | 5-12% | Up to 20% |
| Sleeve Gastrectomy | 1-4% | Up to 5% |
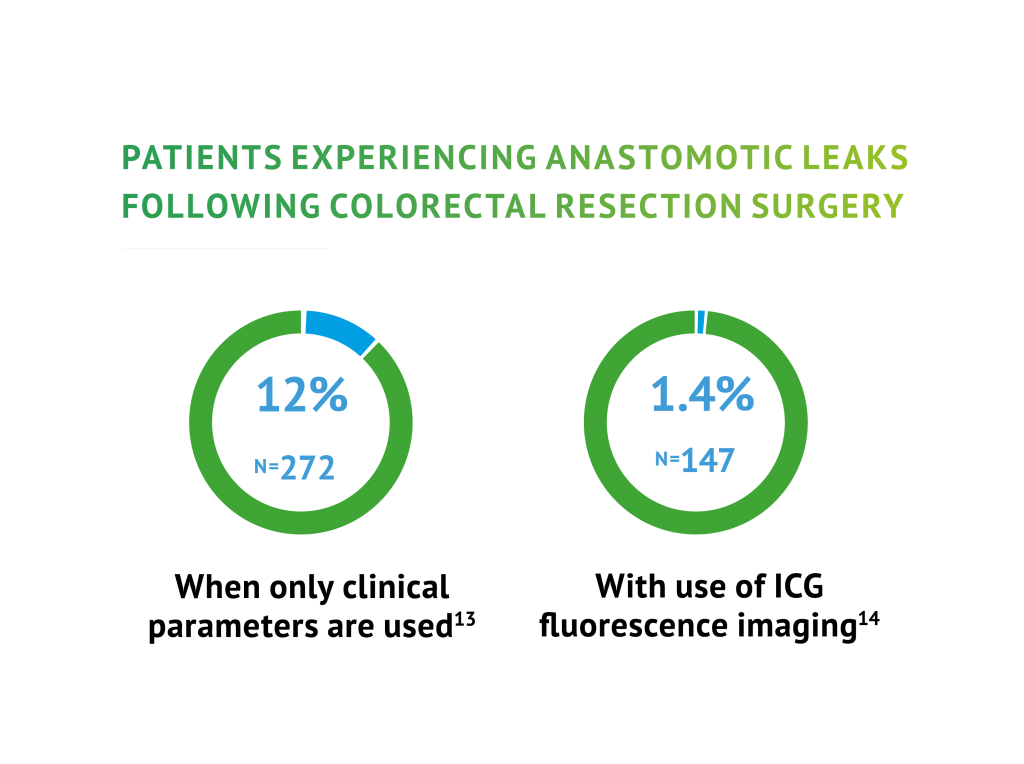
ICG Proven to reduce leak rates in Colorectal Surgery
There is a growing body of evidence that proves the significant value of using ICG in colorectal surgery.
Below is a summary of two recent Clinical Trials proving that ICG is safe, effective and is increasingly viewed as the gold standard in laparoscopic colorectal procedures.
ICG fluorescence imaging during Colorectal Surgery reduces the rate of leaks experienced by patients
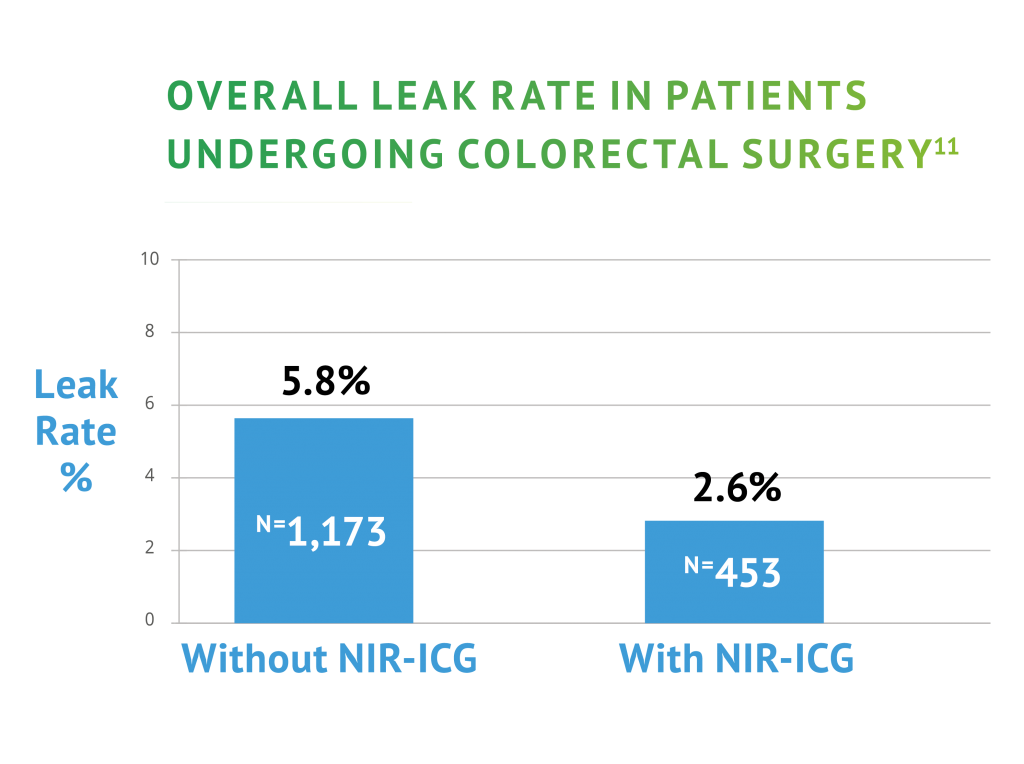
Mortality rates associated with anastomotic leaks, range from 5-17%. Profit margins at hospitals drop by 8% when complications in colon surgeries occur.8
HIGHLIGHTS OF PRESCRIBING INFORMATION
These highlights do not include all the information needed to use IC-Green® (indocyanine green for injection) safely and effectively. See full prescribing information for IC-Green® (indocyanine green for injection).
INDICATIONS AND USAGE
IC-Green® (indocyanine green for injection) is a tricarbocyanine dye, is indicated for:
- Fluorescence imaging of vessels (micro- and macro-vasculature), blood flow and tissue perfusion before, during and after vascular, gastrointestinal, organ transplant, plastic, micro- and reconstructive surgeries, including general minimally invasive surgical procedures, in adults and pediatric patients aged 1 month and older
- Fluorescence imaging of lymph nodes and lymphatic vessels during lymphatic mapping in adults with cervical and uterine cancer
- Ophthalmic angiography in adults and pediatric patients
DOSAGE AND ADMINISTRATION
Visualization of vessels, blood flow and tissue perfusion (2.5 mg/mL solution)
- 1.25 mg to 5 mg by intravenous injection is recommended for a surgical procedure in adults and pediatric patients aged 1 month and older.
- 3.75 mg to 10 mg by intravenous injection is recommended for visualization of perfusion in extremities through the skin for plastic, micro- and reconstructive surgeries in adults.
- Additional doses may be administered. Do not exceed a total dose of 2 mg/kg.
Visualization of extrahepatic biliary ducts in adults and pediatric patients aged 12 years and older (2.5 mg/mL solution)
- 2.5 mg by intravenous injection at least 45 minutes prior to surgery.
- Additional doses may be administered. Do not exceed a total dose of 2 mg/kg.
Lymphatic mapping of cervical and uterine cancer in adults (1.25 mg/mL solution)
- 5 mg interstitially as four 1 mL injections.
Ophthalmic Angiography
- Doses up to 40 mg in 2 mL of sterile water for intravenous injection.
DOSAGE FORMS AND STRENGHTS
For injection: 25 mg of indocyanine green as a lyophilized, green powder for reconstitution in a single-patient-use vial.
CONTRAINDICATIONS
Hypersensitivity to indocyanine green.
WARNINGS AND PRECAUTIONS
Hypersensitivity reactions: Hypersensitivity reactions including anaphylaxis and urticaria have occurred. Always have cardiopulmonary resuscitation personnel and equipment readily available and monitor patients.
ADVERSE REACTIONS
The most common adverse reactions reported are anaphylaxis and urticaria.
To report SUSPECTED ADVERSE REACTIONS, contact Diagnostic Green LLC at 1-844- 424-3784 or FDA at 1-800-FDA-1088 or www.fda.gov/medwatch.
DRUG INTERACTIONS
Interference with Thyroid Radioactive Iodine Uptake Studies: Do not perform radioactive iodine uptake studies for at least one week following the use of IC-Green® (indocyanine green for injection).
See Full Prescribing Information injection techniques.
All references available in the MIS brochure download
Download our MIS Brochure
