Minimally Invasive Surgery (MIS), using small incisions to minimise trauma to normal tissues and adjacent organs, is now the preferred method of undertaking many surgeries.
The global minimally invasive surgical systems market is expected to grow at a CAGR of 10.9% from 2020 to 2025, driven by the rapidly increasing demand from the patients undergoing minimally invasive surgical procedures, increasing surgical need, and the surge in the prevalence of colorectal and other gastrointestinal diseases.1
New technological advancements, such as miniaturisation of surgical equipment and development of surgical robots, have substantially increased the number of minimally invasive surgeries performed across the world.
Laparoscopic Cholecystectomy (Lap Chole)
Key Features
Laparoscopic Cholecystectomy is the gold standard for gall bladder surgery and is one of the most common surgeries undertaken worldwide. In the USA an estimated one million Lap Chole’s are undertaken each year, with an estimated 500,000 in Europe.2
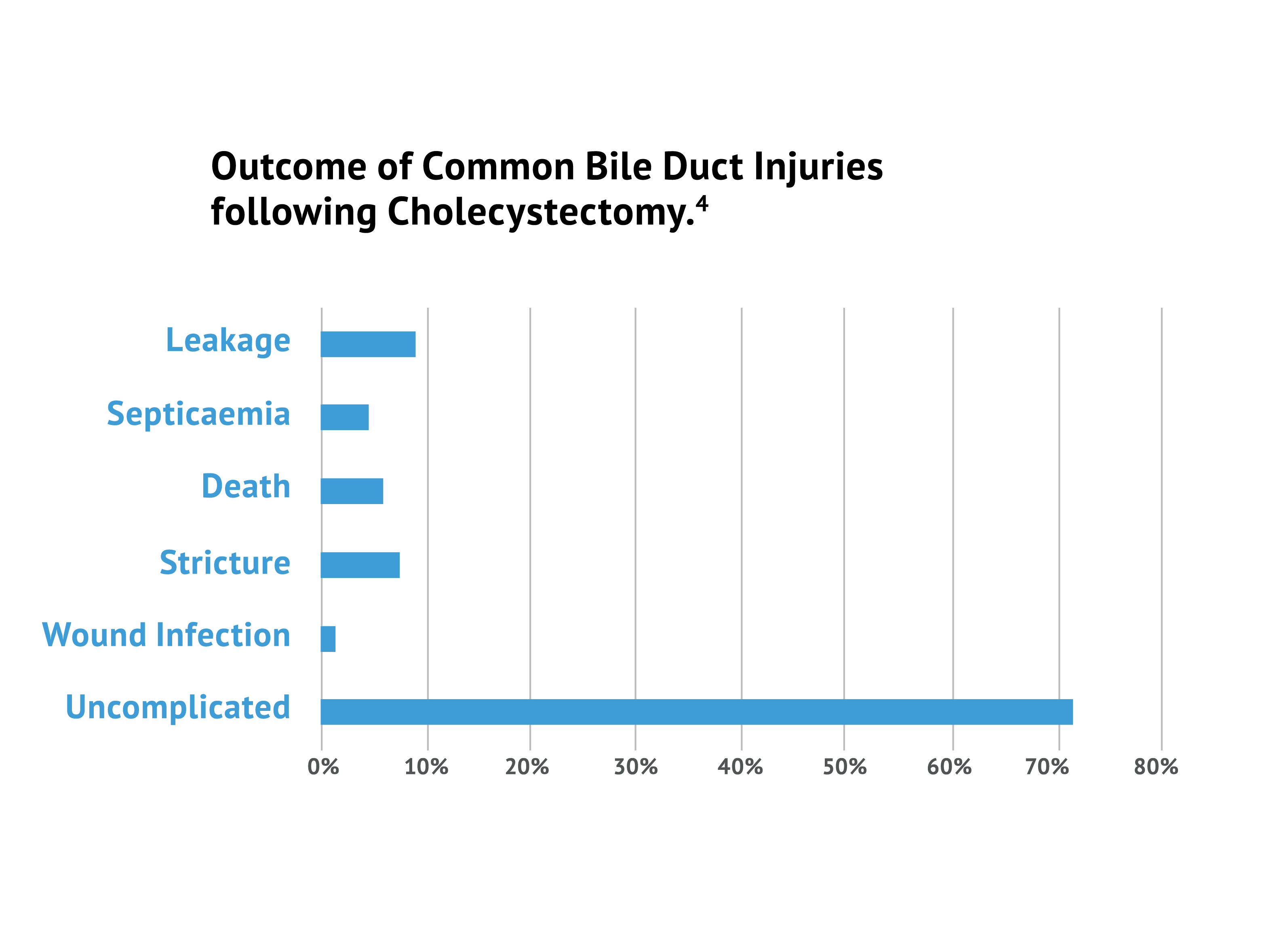
Whilst the incidence of Bile Duct Injury (BDI) is low at 0.5%, due to the considerable amount of surgeries, this becomes quite a significant number with thousands of resultant patients per year thus sustaining BDI’s, with severe and long term implications for their health.2 The primary cause of error in 97% of Lap Chole cases was a visual perception illusion, which is one of the major drawbacks of an MIS approach.3</sup<
ICG fluorescence imaging during Laparoscopic Cholecystectomy (Lap Chole) surgery reduces BDI injuries and improves patient outcomes
The Bile Duct Injury (BDI) rate with laparoscopic cholecystectomy is reported to be 0.5%1, and while relatively low, when injuries occur, they can be catastrophic.2
The primary cause of error in 97% of cases was a visual perception illusion.3
Surgeons had a 3-fold improvement in ability to visualise critical bile duct structures using ICG.4
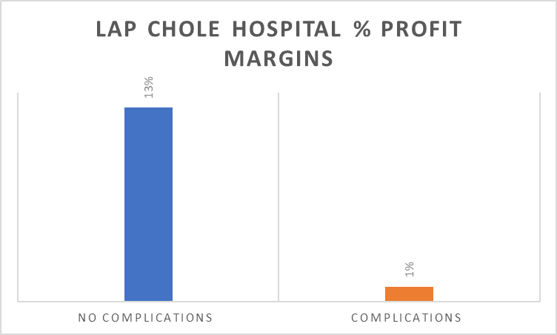
Profit margins at hospitals drop from 13% to 1% when complications in lap chole surgeries occur.5
ICG Guided Cholecystectomy vs X-Ray Cholangiography
X-Ray Cholangiography has been used in the past to overcome this visualisation problem. However it has drawbacks that are not apparent with Indocyanine Green (ICG) use.
ICG Guided Cholecystectomy
X-Ray Cholangiography
Less expensive per patient vs. X-Ray cholangiography.
Requires additional equipment and manpower.
No radiation exposure.
Involves radiation exposure.
Non-invasive and less time consuming.
Requires dissection of the cystic duct which takes procedure time.
Highly specific (anatomy identified at a significantly higher rate) with no learning curve required.
Interpretation relies on the expertise of the surgeon.
Colorectal Surgery
Colorectal surgery frequently involves bowel resection with restoration of the alimentary tract by anastomosis. Indocyanine green (ICG) fluorescence imaging has proven to be an effective tool to assess anastomotic perfusion. Its use for the prevention of anastomotic leaks (AL) has been gaining popularity, with accumulating data on lower leak rates with (ICG) fluorescence guided surgery.9
Most common methods used to evaluate the perfusion status of the colon has been to visually observe the change in colour of the colon wall with the surgeon’s naked eye and to carefully observe the pulse of the colon wall.
However, these methods are subjective and not always accurate.
Reported rates of anastomotic leakage vary from 3-6% in experienced colorectal surgeons and 3-25% overall.10 Combining the use of ICG with a near-infra red (NIR) laparocsopic camera system offers the surgeon the possibility of an objective, real-time assessment of blood flow to the colon.
ICG Proven to reduce leak rates in Colorectal Surgery
There is a growing body of evidence that proves the significant value of using ICG in colorectal surgery.
Below is a summary of two recent Clinical Trials proving that ICG is safe, effective and is increasingly viewed as the gold standard in laparoscopic colorectal procedures.
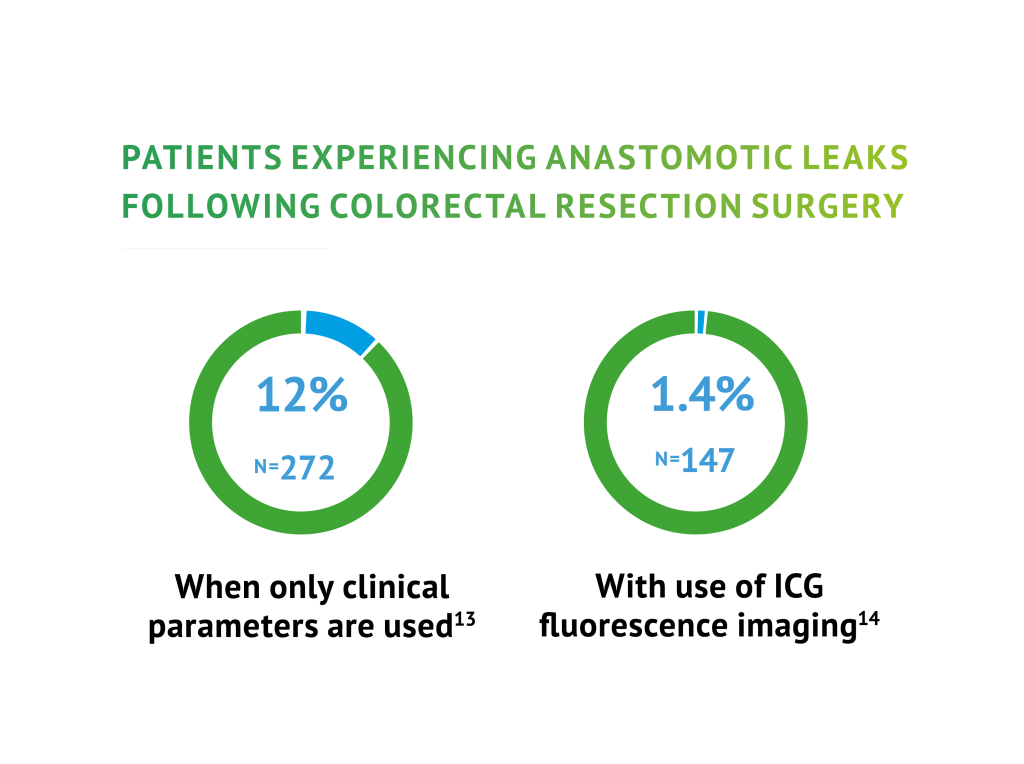
ICG fluorescence imaging during Colorectal Surgery reduces the rate of
leaks experienced by patients
Study
Results
Study Conclusions
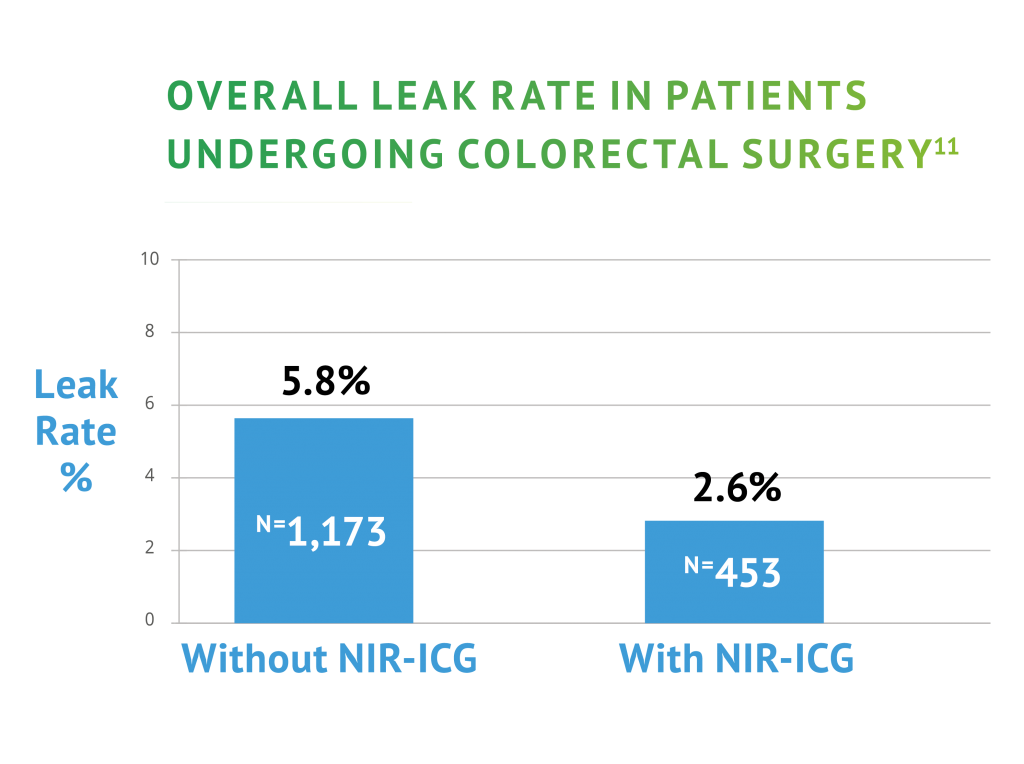
Multicentre phase II trial of
near-infra red imaging in
elective colorectal surgery.11
NIR ICG assessment change in site of bowel
division 29 patients (5.8%) no subsequent
leak rates in these patients. Overall Leak
Rate Standard White light 5.8% versus NIR
ICG 2.6%. Left Anterior Resections Standard
White light 10.7% versus NIR ICG 3%.
NIR-ICG use may change
intraoperative decisions, which may
lead to a reduction in
anastomotic leak.
A study investigating the
Perfusion of Colorectal
Anastomoses using
FLuorescence AnGiography:
results of FLAG trial.12
AL in low anastomoses in ICG FA
14.4% versus 25.7%. ICG FA led to
changes in the transection line in
almost 20% of patients.
ICG FA is well tolerated and
simple to perform. Significant
reductions in anastomotic leakage were
observed in patients following low
anterior resection.
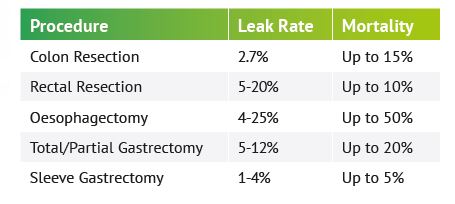
Mortality rates associated with anastomotic leaks, range from 5-17%.15
Profit margins at hospitals drop by 8% when complications in colon surgeries occur.8