
Use of Verdye (ICG) in
Liver
With primary liver cancer and colorectal liver metastases amongst the most common leading causes of cancer-related deaths worldwide, surgery represents one of the main treatments to
obtain the best results in overall and disease free survival.1 Verdye (Indocyanine Green, ICG) in recent years has experienced increased interest in use for its clearance parameters as a dynamic
assessment of liver function both in medical and surgical settings.2 ICG is used routinely to evaluate hepatic function and liver blood flow.3 It is one of the most common and easy-to-use tests for the perioperative dynamic assessment of liver function in cases of major liver surgery (resective surgery and liver transplantation) and in the intensive care unit.
Use of Verdye in Liver Function Diagnostics include:
- Measurement of excretory function of the liver Measurement of liver blood flow
- Verdye (Indocyanine Green (ICG)) is a tricarbocyanine dye with both hydrophilic and lipophilic properties.
While numerous clinical parameters are used to assess a patient’s liver function, the ICG test is the gold standard and is the only established test for estimating true global liver function.4
Assessment of dynamic liver function is crucial in the pre-operative preparation of those who require extensive liver resections, liver transplants and also to monitor liver function in a post-operative setting.
The ICG clearance or the elimination test is the most widely used quantitative liver function test. Following the administration of ICG I.V., serial blood samples are collected at 5, 15, 20, 25 & 30 mins. The ICG blood levels fall exponentially for about 20mins, by which time approximately 97% of the ICG is excreted. After processing the samples, the ICG-R15 (at 15 mins) is determined as a percentage.

QUANTITATIVE MEASUREMENT
- ICG Retention 15mins (ICG-R15) (Normal <10%)
- Pulse Dye Densitometry – LiMON device
- ICG Plasma Disappearance Rate (ICG-PDR) (Normal > 18%/min)5
ICG CLEARANCE TESTS
- Pre and post Liver Resections
- Pre and post Liver Transplant Surgery
- Acute Liver Failure (ICU setting)
VERDYE USE IN TREATMENT FOR HEPATOCELLULAR
CARCINOMA (HCC)
Over the last few decades, imaging technologies in hepatobiliary (HPB) surgery have become
indispensable tools for liver surgeons. The ICG fluorescence imaging (FI) technique helps to
guide the hepatic surgical procedures and provides the surgeon with real-time visualisation of
the fluorescent structures of interest that would be invisible under conventional white light.
The extrahepatic bile duct anatomy and liver tumours can be emphasised, and hepatic segments
highlighted, based on the fluorescence property of ICG and its biliary excretion.

COLORECTAL LIVER METASTASES AND LIVER TRANSPLANT USE OF ICG
Additionally, a recent retrospective multi-center analysis of 174 patients showed that the use of ICG identifies significantly more and smaller tumours during colorectal liver metastases (CRLM) resection.8 For liver transplantation, use of ICG has shown to be the best curative treatment of chronic liver diseases/HCC/acute liver failure. Increasing the use of marginal grafts can lead to increased incidence of primary non-function (PNF) after transplantation with few early predictors available for PNF. By undertaking quantitative assessment of intra-operative ICG fluorescence on the graft, a 2020 study has shown that it was feasible to predict graft survival at three months with good sensitivity and specificity.9
Italy snapshot of LLR surgeries in practice
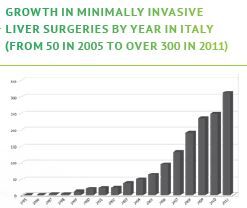
- LLR represents 10.3% of all Liver Resections (1677 cases)
- Malignant lesions 72.5% (1085 cases)
- 56% – Hepatocellular Carcinoma (HCC)
- 28% – Colorectal Liver Metastases (CRLM)
- Overall mortality 0.2%
- Mean length of stay is five days
SUMMARY OF VERDYE (ICG) IN LIVER SETTING
- Liver Function Assessment – Pre & Post Op
- Intra-operative identification of anatomic liver segments
- After reconstruction of hepatic vessels – assessment of liver inflow and outflow of blood
- Useful for real-time detection of bile leaks during liver resection
- Visualisation of Liver Tumours (HCC & CRLM)
VERDYE USE – BENEFITS TO THE SURGEON
- Real time visualisation of anatomical structures
- Simple method to evaluate hepatic function
- Allows for safe use of marginal liver grafts
- Easy to use test for dynamic assessment of liver blood flow
- Helps identify more and smaller colorectal tumours
- Quantitative liver function test
Note: All references are available in our brochure download
For full details download our Liver Brochure
