Background: Although the usefulness of indocyanine green fluorescence imaging (ICG-FI) for anastomotic perfusion has been demonstrated in randomized controlled trials, the incidence of anastomotic leakage is not sufficiently low, even in patients using ICG. Because blood flow assessment using ICG is not completely objective, the objectivity of blood flow evaluation is expected to improve by quantification of fluorescence signals. This study aimed to clarify the efficacy of quantitative assessment of blood flow using ICG-FI with the SPY-QP software program in rectal cancer surgery.
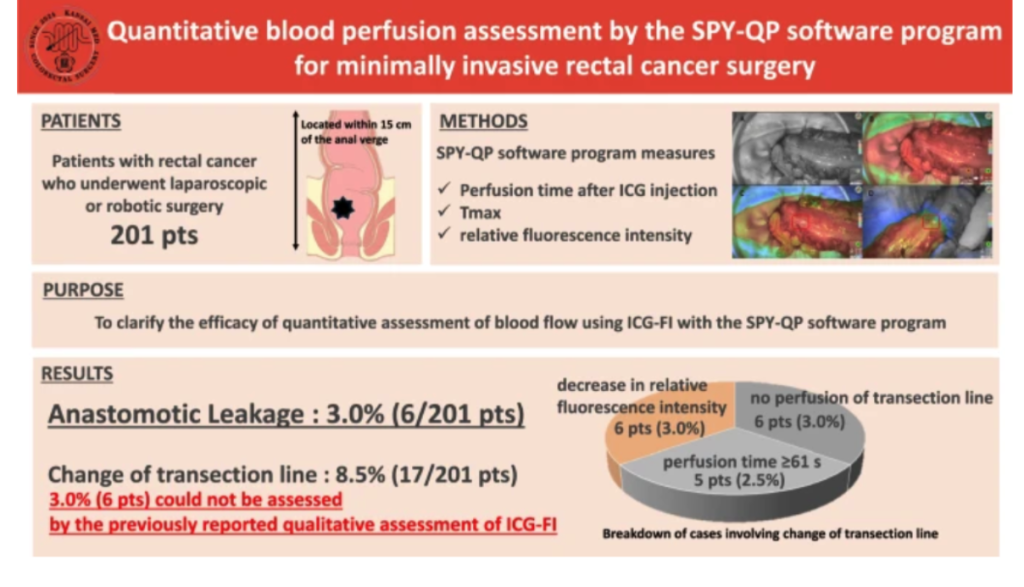
Methods: This retrospective study included 201 patients with rectal cancer who underwent laparoscopic or robotic surgery for rectal cancer using SPY-QP at two tertiary referral centers between December 2021 and November 2024. We recorded the time from the onset of fluorescence at the most proximal bowel wall to the plateau (Tmax) and the relative fluorescence intensity and assessed its correlation with the occurrence of AL.
Results: Among 201 patients, anastomotic leakage occurred in 6 patients (3.0%). Tmax in the SPY-QP was positively correlated with the time for fluorescence perfusion after ICG injection (correlation coefficient = 0.55). The point of the proximal colon transection line was shifted by quantification of ICG-FI in 17 patients (8.5%). Of these, 6 patients (3.0%) with a decrease in relative fluorescence intensity of the planned transection line could not be assessed by a qualitative assessment of ICG-FI. The relative fluorescence intensities of patients without anastomotic leakage were ≥ 60% for Tmax ≤ 30 s and ≥ 70% for Tmax 31-40 s.



